
A Guide to ACL and PCL Ligament Sprains and Their Management: A Physiotherapy Perspective
At Connect Physiotherapy & Exercise, we often encounter patients dealing with discomfort and pain in the knee because of injury to one or more of the cruciate ligaments. Often this injury is simply referred to as a knee sprain. These injuries, especially those involving the anterior cruciate ligament (ACL), are a source of knee pain that can significantly impact an individual’s mobility and quality of life.
A ligament sprain occurs when the forces acting on the tissue exceed its viscoelastic capacity. This means the tissue is stretched beyond its ability to return to its original shape. Imagine stretching a rubber band too far – it will reach a breaking point and snap. In the context of the knee, this can involve the ACL or the posterior cruciate ligament (PCL).
An ACL sprain happens when the tibia (the larger bone in your lower leg) moves forward on the femur (your thigh bone). This is also often coupled with a rotational force as well. On the other hand, a PCL sprain occurs when the tibia moves backwards on the femur. Think of a football player being tacked from the front, below the knee, forcing the tibia backwards on the femur. These movements can destabilize the knee and lead to pain and other symptoms.
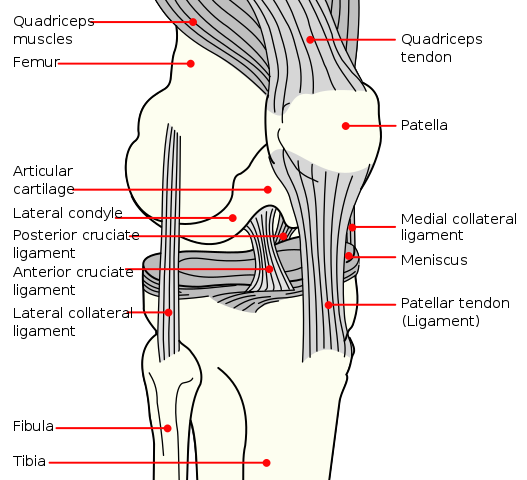
Mysid, Public domain, via Wikimedia Commons
Causes of Cruciate Ligament Sprains
The knee is a complex joint, and its position in the kinetic chain – the interconnected group of body segments that work together to perform movement – makes it particularly susceptible to injury. The knee’s inherent mobility and reliance on the ligamentous structures surrounding the joint for stabilization increases the likelihood of injury following hip, ankle, or knee injuries.
ACL sprains can be either traumatic or non-contact and tend to be seen more in athletes, particularly those between the ages of 14 and 29 who engage in high levels of vigorous activity. These injuries typically involve mechanisms that include sudden stops, changes in direction, hyperextension, and direct impact to the knee. Interestingly, non-contact injuries are more common than contact injuries. Some estimates have non-contact injuries accounting for 70% of ACL tears.
Research suggests that female athletes are more prone to ACL injuries due to factors such as tissue property differences, menstrual cycle hormonal variations, and altered knee mechanics.
The Impact of a Cruciate Ligament Sprain on the Knee
A sudden or violent twisting or wrenching of the knee joint can cause an ACL or PCL sprain. This causes the tibia to move in relation to the femur, leading to instability in the knee. The severity of the injury typically dictates the degree of instability; more severe sprains can result in more instability and potentially in more directions.
Individuals with ACL deficient knees have an increased risk of articular cartilage damage, meniscal degeneration, and functional instability. This is due to the increased laxity at the knee joint post injury as well as deconditioning and altered movement patterns that can develop.
Recognizing the Symptoms
Common symptoms of cruciate ligament sprains include knee pain, feelings of instability, loss of range of motion, and swelling in the knee. In ACL injuries, the patient often feels or hears a pop and is unable to continue with their activity.
In PCL injuries, symptoms may include moderate stiffness of the knee, medial joint line pain, and retropatellar pain. However, it’s important to note that the PCL is the strongest and least frequently injured knee ligament, involved in only 3-20% of all knee injuries.
Managing Cruciate Ligament Sprains
When it comes to treating cruciate ligament sprains, the approach can vary depending on the severity of the injury and the patient’s lifestyle. The general approach to the acute inflammatory phase of a cruciate ligament sprain is PRICE MM (Protection, Rest, Ice, Compression, Elevation, Medication, and Modalities). Following this, first and second-degree sprains are usually treated conservatively, while third-degree sprains can be treated surgically or conservatively.
The main goals of conservative intervention are to decrease swelling and inflammation, restore range of motion of the knee, increase the strength of the quadriceps and hamstrings, and work on balance and functional activities. Bracing may be indicated but is patient specific.
For patients who undergo surgery, early motion post-surgery can help avoid arthrofibrosis problems, and weight-bearing may decrease patellofemoral pain post-surgery. For PCL injuries, it’s important to avoid active hamstring exercises and movements that would translate the tibia posteriorly on the femur. Early, protected range of motion is required.
Exercise and Manual Therapy
Exercise prescription will be based on the severity of the sprain and stage of healing, along with the patient’s current level of strength, range of motion (ROM), pain, and functional activities. Examples of exercises include heel slides for increasing ROM, standing knee bends/squats and hamstring curls for strength, single leg stance for balance, and deceleration drills for functional activities.
There is limited evidence for the use of manual therapy to treat cruciate ligament injuries. However, after surgical ACL repair, passive, active-assisted, and active stretching may be prescribed to stretch the knee into flexion to prevent a ROM restriction.
Cruciate ligament sprains, particularly ACL injuries, are a cause of knee pain that can significantly impact an individual’s ability to participate in physical activities and sport. Understanding the risk factors, the pathophysiology, and the symptoms of these injuries is crucial in seeking timely treatment and preventing further damage.
At Connect Physiotherapy & Exercises in Edmonton, we believe in the power of knowledge and active participation in one’s health. If you’re experiencing symptoms of a knee injury, we invite you to reach out for a consultation. Early intervention can make a significant difference in your recovery journey.
*Remember, while knowledge is power, self-diagnosis and treatment can be risky. While this blog provides useful information, it’s essential to see a trained professional for proper diagnosis and management. Every person is unique, and so is their recovery journey. At Connect Physiotherapy & Exercise, we’re all about personalized care. Let us help you navigate your path to recovery
References:
Agur, A.M.R., Dalley, A.F., & Moore, K.L.(2010). Lower extremity. Clinically oriented anatomy (6th ed.) (pp. 634-645, 662-663). Philadelphia, PA: Lippincott, Williams, & Wilkins.
Kramer, L.C., Denegar, C.R., Buckley, W.E., & Hertel, J. (2007). Factors associated with anterior cruciate ligament injury: history in female athletes. Journal of Sports Medicine and Physical Fitness, 47(4), 446-454. doi:10.1136/bjsm.2009.059139
Magee, D.J. (2014). Knee. Orthopedic physical assessment (6th ed.) (pp. 765-877). St. Louis, MO: Elsevier.
Magee, D.J. & Sueki, D. (2011). Knee. Orthopedic physical assessment atlas and video: selected special tests and movements (pp. 339-409). St. Louis, MO: Elsevier.
Smith, M.A., Smith, T., & Kosko, P. (2014). Anterior Cruciate Ligament Tears: Reconstruction and Rehabilitation. Orthopedic Nursing, 33(1), 14-24.
Yabroudi, M.A., & Irrgang, J.J. (2013). Rehabilitation and return to play after anatomic anterior cruciate ligament reconstruction. Clinical Sports Medicine, 32, 165-175.

