
Acromioclavicular Joint Separation: What You Need to Know
A Closer Look at the AC Joint
At the top of our shoulder lies the acromioclavicular (AC) joint, a pivotal point that facilitates many of our daily movements. When this joint is injured, it can result in pain, especially when lifting the arm or reaching across the body. In this guide, we’ll explore AC joint separation, its causes, symptoms, and the role of physiotherapy in its management.
What is Acromioclavicular Joint Separation?
The AC joint is where the scapula’s acromion process meets the clavicle’s lateral end. Think of it as a bridge connecting two crucial bones in your shoulder. An AC separation indicates a disruption in this bridge, leading to tissue damage.
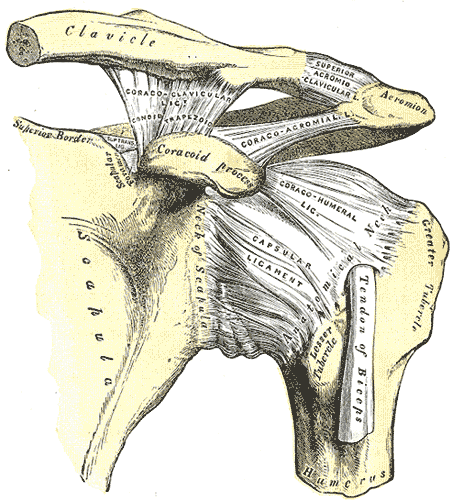
Shoulder Joint, Henry Vandyke Carter, Public domain, via Wikimedia Commons
AC Joint Injury Causes and Classification
A primary cause of AC separation is a traumatic force, such as getting hit into the boards while playing hockey or a fall on an outstretched hand. This force can deeply affect the tissues surrounding the AC joint.
To gauge the severity of an AC joint separation, healthcare professionals often use the Rockwood Classification. Here’s a basic breakdown:
- Type I:
- A mild injury with the main ligament slightly stretched. Treatment: Wearing a sling for support.
- Type II:
- The main ligament is torn, but the secondary one is slightly stretched. A visible step might be noticeable. Treatment: Typically a sling.
- Type III:
- Both main and secondary ligaments are torn, with a more pronounced step. Treatment varies, but a sling is often recommended.
- Type IV:
- A severe injury with the bone pushed in an abnormal direction. Surgery is typically needed.
- Type V:
- An even more severe injury with a pronounced shoulder droop. Surgery is the usual treatment.
- Type VI:
- A rare and very severe injury with the bone pushed downward. Surgery is typically necessary.
The Mechanics of AC Joint Injuries
A hit or fall on the shoulder pushes the acromion process away from the clavicle, straining the surrounding structures. A fall on an outstretched arm drives the humerus into the acromion, pushing it away from the fixed clavicle.
Diagnosis and Symptoms
Radiographs, or X-rays, are the primary method for diagnosing AC separation. Often they are done holding a weight in hand to help determine the separation degree. Specific orthopedic tests can reproduce pain over the AC region, indicating the injury’s presence in lower degree injuries.
Key symptoms include:
- Localized pain around the AC joint.
- A correlation between pain severity and the separation degree.
- A visible step in higher grade injuries.
Physiotherapy Treatment Approach
For Grade I and II AC separations, conservative management is the primary approach. Grade III separations usually involve conservative treatment for 6-12 weeks before considering surgery. Grades IV to VI often require surgical procedures due to extensive tissue damage.
If surgery is done, post-operative care starts with immobilization and protecting the joint in specific positions. Once able strength exercises, progressing based on the healing phase and patient symptoms. Exercises focusing on proprioception and neuromuscular control are essential, especially after immobilization.
Exercise and Manual Therapy
For patients with a stable AC joint injury, manual therapy can be offered to help manage pain and tension in the surrounding muscles. As the condition progresses, deep transverse frictions can be introduced to enhance the healing process. Pain-free PNF patterns (banded shoulder strength exercises) are also beneficial in aiding the return to functional activities. The end stage of rehab will work on building strength and control around the joint through basic strength exercises. If the end goal is returning to sport, and more specifically collision or contact sports, additional testing may be needed to ensure the joint can tolerate the impact.
When working your way back to typical exercises it’s essential to exercise caution during the recovery process. Activities that jolt or distract the joint, such as running, jogging, and rowing, should be avoided early on. Loading the arm in distraction, like performing dumbbell exercises in standing for the upper extremity, can disrupt the newly forming collagen. This disruption might prolong healing times and cause the healing to occur in a lengthened position. Working with a qualified health professional can help guide you through this process.
Your Recovery Journey in Edmonton
Shoulder injuries, including those involving the AC joint, should be assessed and treated by a qualified health professional. At Connect Physiotherapy & Exercise in Edmonton, our team is dedicated to guiding you through your recovery journey. If you suspect an AC joint separation or experience shoulder pain, reach out to us. Book today with Connect Physiotherapy & Exercise for more information or to schedule an appointment!
*Remember, while knowledge is power, self-diagnosis and treatment can be risky. While this blog provides useful information, it’s essential to see a trained professional for proper diagnosis and management. Every person is unique, and so is their recovery journey. At Connect Physiotherapy & Exercise, we’re all about personalized care. Let us help you navigate your path to recovery.
References:
Johnson, R. (2011). Acromioclavicular injuries. In Micheo, W (Eds.) Musculoskeletal, sports, and occupational medicine (pp.11-13).
Mazzocca, A. (2007). Evaluation and Treatment of Acromioclavicular Joint Injuries. American Journal Of Sports Medicine, 35(2), 316-329.
Phyllis, M., & Timothy, D. (n.d). The acromioclavicular joint. Primary Care: Clinics In Office Practice, 31(Sports Medicine, Part I), 857-866.
Reid, D., Poison, K., & Johnson, L. (2012). Acromioclavicular Joint Separations Grades I- III: A Review of the Literature and Development of Best Practice Guidelines. Sports Medicine, 42(8), 681-696.
Photo accessed at: https://commons.wikimedia.org/wiki/File:Gray326.png

